Yerba maté is a large Amazonian tree. Its leathery leaves are dried and consumed as a tea similarily to green and black tea. It's a potent source of caffeine and antioxidants...
Ashwagandha (Withania somnifera)
Rhodiola (Rhodiola rosea)

Rhodiola Summary
Rhodiola was made famous by some earlier research done by Russian scientists in the 1960's. Although a lot of this research still hasn't been released to the public, there has been a lot of new studies put forward to make up for this loss.
Rhodiola is well revered as an adaptogen for treating fatigue, cognitive decline, depression, and for athletic enhancement. It's considered to be a mild stimulant, though it doesn't produce the "wired" feeling many other stimulants produce. It increases energy levels and makes us more tolerant of stressful situations.
Although there is still a lot of research lacking, we know that Rhodiola can reduce cortisol levels in the body after exposure to stress, however, the details on how this interaction exists is still not well understood. There is also a great deal of confusion around which chemicals are active in the herb, some studies showing the rosavins, others tyrosol and the rhodiolasides.
As a result, each manufacturer tends to have a preference for one chemical group over the other in their products.
What is Rhodiola Used For?
*Rhodiola rosea* is mainly used for its adaptogenic qualities, especially those specific to lowering cortisol levels. It's reliable for improving fatigue in debilitated or chronically fatigued people, as well as those experiencing generalized adaptive disorder, depression, or acute periods of extreme stress.
Rhodiola is a popular nootropic additive for increasing focus and mental endurance and is popular among athletes for increasing physical endurance as well.
Herb Details: Rhodiola
Weekly Dose
- (1:2 Liquid Extract)
20–40 mL - View Dosage Chart
Part Used
- Root/Rhizome
Family Name
- Crassulaceae
Distribution
- Northern climates of North America, Asia, and Europe
Herbal Actions:
- Adaptogen
- CNS Stimulant (mild)
- Antidepressant
- Cardioprotective
- Nootropic
Constituents of Interest
- Rosavin
- Tyrosol
- Salidroside
- Rhodiolaside
Common Names
- Rhodiola
- Rose Root
- Arctic Root
- Golden Root
- King's Crown
CYP450
Unknown
Duration of Use
- Long-term use of rhodiola is acceptable.
Botanical Information
Although Rhodiola rosea is the preferred species used, there are many species used in various indigenous medical systems such as Rhodiola alterna, Rhodiola brevipetiolata, Rhodiola crenulata, Rhodiola kirilowii, Rhodiola quadrifida, Rhodiola sachalinensis, and Rhodiola sacra.
The Crassulaceae family contains 34 genera and 1400 species. Most of the plants in this family can be found in colder climates.
Another medicinal species in this family is Kalanchoe.
Habitat Ecology, & Distribution:
Rhodiola grows at high altitude, mountainous regions of Europe, Asia, the Arctic, and North America.
Pharmacology & Medical Research
+ Altitude Sickness
Salidroside and Tyrosol from Rhodiola cerrulea extracts have been shown to regulate AMPK [11], which plays a major role in energy homeostasis [10]. It was also shown to maintain sodium channel transport by preserving NA+, K+, ATPase activity. The authors concluded that this mechanism may be responsible for Rhodiolas ability to reduce the symptoms of altitude sickness, particularly HAPE [11].
+ CNS Stimulant
Numerous clinical trials have demonstrated the CNS stimulating activity of Rhodiola rosea [8] based on various cognitive and fatigue scores.
Other studies have found the use of rhodiola at varying doses inconclusive as a stimulant [7].
+ Memory & Cognitive Performance
Rhodiola extracts have been shown in animal models to improve learning capacity and short/long-term memory in animals trained to perform certain tasks [2].
Rhodiola has been shown to inhibit monoamine oxidase (both MAO-A and MAO-B) in animal studies [4].
+ Depression
MAO-A inhibitors are effective in the treatment of depression [20]. Rhodiola has been shown to inhibit MAO-A & B in animal studies [4]. Other animal studies investigating the use of rhodiola on depression has shown a non-dose dependent improvement on depression scores in mice, which is due to the tyrosin and rhodiolaside content specifically [16, 18, 19].
A randomized double-blind clinical trial using a standardized Rhodiola rosea extract showed a significant antidepressant activity in the treatment group compared to placebo. This was based on various depressive symptoms including insomnia, emotional instability, and somatization. [17].
+ Stress And Fatigue (Adaptogenic)
A group of 56 healthy physicians in a double-blind randomized clinical trial were either given Rhodiola rosea extracts or placebo control for 2 weeks. Physicians were chosen based on criteria that investigated the likelihood that these physicians would experience mental exhaustion during a normal shift. A series of tasks were then given after each night shift to investigate any changes on mental fatigue as measured by a set of complex tasks. All of the physicians treated with Rhodiola rosea were noted to show improved test scores compared to those not treated with the herb. These effects were observed to be most active after two weeks of use, and not a single adverse reaction was reported during the study. [3].
Another study investigating the mental and physical effects of a long term, low dose (SHR-5 50 mg) on students during examination periods found significant improvements on test scores among the treatment group [9]. They were looking for the presence of mental and physical fatigue indications. The only test that showed no improvement in this study was the tapping test (muscular activation).
A study investigating the effects of Rhodiola rosea on free cortisol levels in chronically fatigues patients noted a reduction in cortisol levels after just a single treatment, and significantly after a 28-day course of treatment [21]. Rhodiola was also shown to reduce serum blood levels of cortisol after a stressful event in rabbits [22].
Animal research has shown that Rhodiola rosea extracts can reduce the expression of c-Fos in the hypothalamus of rats [23]. The expression of this gene is considered to be a valuable marker for identifying the activation of cells in the central nervous system associated with the stress response [24]. This suggests the mechanism of action for Rhodiola rosea on reducing cortisol levels is the result of HPA modulation in the hypothalamus, such as increasing feedback sensitivity and therefore reducing overall CRH release rather than acting directly on the adrenal glands.
+ Withdrawal
A Rhodiola rosea extract was shown to improve withdrawal symptoms in mice, with a noted increase in 5HT activity in treated animals. [1].
Clinical Applications Of Rhodiola:
Rhodiola serves as a reliable adaptogen with little to no side effects noted in any of the studies listed. It's useful for those suffering from high-stress conditions, chronically fatigued, or depressed.
This herb is also useful for increasing athletic performance in athletes and reducing the chances of being affected by altitude sickness when traveling above 2500 meters.
Cautions:
Caution when using Rhodiola with mania as the mental stimulation may produce negative side effects.
Recent Blog Posts:
Featured








References
Mannucci, C., Navarra, M., Calzavara, E., Caputi, A. P., & Calapai, G. (2012). Serotonin involvement in Rhodiola rosea attenuation of nicotine withdrawal signs in rats. Phytomedicine, 19(12), 1117-1124. [animal studies]
Petkov, V. D., Yonkov, D., Mosharoff, A., Kambourova, T., Alova, L., Petkov, V. V., & Todorov, I. (1986). Effects of alcohol aqueous extract from Rhodiola rosea L. roots on learning and memory. Acta physiologica et pharmacologica Bulgarica, 12(1), 3-16. [animal studies]
Darbinyan, V., Kteyan, A., Panossian, A., Gabrielian, E., Wikman, G., & Wagner, H. (2000). Rhodiola rosea in stress induced fatigue—a double blind cross-over study of a standardized extract SHR-5 with a repeated low-dose regimen on the mental performance of healthy physicians during night duty. Phytomedicine, 7(5), 365-371. [RCT]
Van Diermen, D., Marston, A., Bravo, J., Reist, M., Carrupt, P. A., & Hostettmann, K. (2009). Monoamine oxidase inhibition by Rhodiola rosea L. roots. Journal of ethnopharmacology, 122(2), 397-401. [animal studies]
Ganzera, M., Yayla, Y., & Khan, I. A. (2001). Analysis of the marker compounds of Rhodiola rosea L.(golden root) by reversed phase high performance liquid chromatography. Chemical and pharmaceutical bulletin, 49(4), 465-467. [chemical analysis]
Panossian, A., Wikman, G., & Sarris, J. (2010). Rosenroot (Rhodiola rosea): traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine, 17(7), 481-493. [review article]
Shevtsov, V. A., Zholus, B. I., Shervarly, V. I., Vol'skij, V. B., Korovin, Y. P., Khristich, M. P., ... & Wikman, G. (2003). A randomized trial of two different doses of a SHR-5 Rhodiola rosea extract versus placebo and control of capacity for mental work. Phytomedicine, 10(2), 95-105. [RCT]
Panossian, A., & Wagner, H. (2005). Stimulating effect of adaptogens: an overview with particular reference to their efficacy following single dose administration. Phytotherapy Research, 19(10), 819-838. [Review]
Spasov, A. A., Wikman, G. K., Mandrikov, V. B., Mironova, I. A., & Neumoin, V. V. (2000). A double-blind, placebo-controlled pilot study of the stimulating and adaptogenic effect of Rhodiola rosea SHR-5 extract on the fatigue of students caused by stress during an examination period with a repeated low-dose regimen. Phytomedicine, 7(2), 85-89. [RCT].
Lee, S. Y., Shi, L. S., Chu, H., Li, M. H., Ho, C. W., Lai, F. Y., ... & Chang, T. C. (2013). Rhodiola crenulata and its bioactive components, salidroside and tyrosol, reverse the hypoxia-induced reduction of plasma-membrane-associated Na, K-ATPase expression via inhibition of ROS-AMPK-PKCξ pathway. Evidence-Based Complementary and Alternative Medicine, 2013. [in vitro].
Reznick, R. M., & Shulman, G. I. (2006). The role of AMP‐activated protein kinase in mitochondrial biogenesis. The Journal of physiology, 574(1), 33-39.
Kerharo, J., & Adam, J. G. (1974). La pharmacopée sénégalaise traditionnelle: plantes médicinales et toxiques. (Pharmacopoeia).
Steinegger, E., & Hansel, R. (1992). Pharmakognosie 5 Aufl. Kap 6.2. 1. Freie Phenolcarbonsauren Springer Verlag Berlin. (Pharmacopoeia).
Hjaltalin, O. J. (1830). Islenzk grasafrædi. Koben havn.
insert
Kurkin, V. A., Dubishchev, A. V., Ezhkov, V. N., Titova, I. N., & Avdeeva, E. V. (2006). Antidepressant activity of some phytopharmaceuticals and phenylpropanoids. Pharmaceutical Chemistry Journal, 40(11), 614-619.
Darbinyan, V., Aslanyan, G., Amroyan, E., Gabrielyan, E., Malmström, C., & Panossian, A. (2007). Clinical trial of Rhodiola rosea L. extract SHR-5 in the treatment of mild to moderate depression. Nordic journal of psychiatry, 61(5), 343-348.
Perfumi, M., & Mattioli, L. (2007). Adaptogenic and central nervous system effects of single doses of 3% rosavin and 1% salidroside Rhodiola rosea L. extract in mice. Phytotherapy Research, 21(1), 37-43.
Panossian, A., Nikoyan, N., Ohanyan, N., Hovhannisyan, A., Abrahamyan, H., Gabrielyan, E., & Wikman, G. (2008). Comparative study of Rhodiola preparations on behavioral despair of rats. Phytomedicine, 15(1-2), 84-91.
Priest, R. G., Gimbrett, R., Roberts, M., & Steinert, J. (1995). Reversible and selective inhibitors of monoamine oxidase A in mental and other disorders. Acta Psychiatrica Scandinavica, 91(s386), 40-43.
Olsson, E. M., von Schéele, B., & Panossian, A. G. (2009). A randomised, double-blind, placebo-controlled, parallel-group study of the standardised extract shr-5 of the roots of Rhodiola rosea in the treatment of subjects with stress-related fatigue. Planta medica, 75(02), 105-112.
Panossian, A., Hambardzumyan, M., Hovhanissyan, A., & Wikman, G. (2007). The adaptogens Rhodiola and Schizandra modify the response to immobilization stress in rabbits by suppressing the increase of phosphorylated stress-activated protein kinase, nitric oxide and cortisol. Drug target insights, 2, 117739280700200011.
Xia, N., Li, J., Wang, H., Wang, J., & Wang, Y. (2016). Schisandra chinensis and Rhodiola rosea exert an anti-stress effect on the HPA axis and reduce hypothalamic c-Fos expression in rats subjected to repeated stress. Experimental and therapeutic medicine, 11(1), 353-359.
Luckman, S. M., Dyball, R. E., & Leng, G. (1994). Induction of c-fos expression in hypothalamic magnocellular neurons requires synaptic activation and not simply increased spike activity. Journal of Neuroscience, 14(8), 4825-4830.
Stevia (Stevia rebaudiana)
Cannabis (Cannabis sativa/indica)

Cannabis Overview
Cannabis is well known for its psychoactive effects, causing temporary changes in visual and auditory perception.
The cannabis plant is also a rich source of medicinal compounds. Cannabinoids related to THC exert medicinal action through the endocannabinoid system — a critical component of homeostasis.
Many of these cannabinoids aren't psychoactive, and wont produce the 'high' associated with the plant in their isolated forms.
Compounds like CBD, have become especially popular as a supplement recently for its broad medicinal benefits.
There are plenty of uses for cannabis — however, product selection, strain choice, and cannabinoid profiles make a big difference in the effects produced by the plant. It's important to use the right type of cannabis for the job.

What is Cannabis Used For?
Using cannabis as medicine poses challenges due to the large variety of effects each cannabinoid possesses. Different cannabinoid and terpene ratios can produce different effect profiles.
The plant has many claimed benefits, and though a lot of them can be validated, it's not a miracle plant.
Cannabis is especially reliable for a few key symptoms:
- Lowering various forms of inflammation
- Improving microbiome diversity (through CB2 receptor activity)
- Reducing nervous excitability
- Reducing convulsions
- Improving sleep onset and maintenance
- Lowering pain
Using cannabis as medicine should be attempted with caution due to the degree of variability the plant produces in terms of effect profile. What this means is that some cannabis extracts will make symptoms like anxiety worse, while others can dramatically improve it.
Choosing the right strain or extract is of the utmost importance when using cannabis as medicine.
The effects of cannabis can be contradictory:
- It's both a stimulant and a sedative
- It increases appetite, and suppresses it
- It increases immune activity, and suppresses inflamamtion
These effects all contradict themselves in most cases. The reason this happens is because the cannabinoids work through a regulatory pathway (endocannabinoid system) rather than on a particular organ function.
It's similar to how adaptogens like ginseng, ashwagandha, or reishi produce often contradictory or bidirectional results.
+ Indications
- Anorexia
- Cancer
- Crohn's disease
- Dystonia
- Epilepsy
- General anxiety disorder
- Glaucoma
- Gout
- Insomnia
- Menstrual cramping
- Multiple Sclerosis
- Neuropathic pain
- Osteoarthritis
- Rheumatoid Arthritis
- Schizophrenia (Caution)
- Social anxiety disorder
- Substance abuse/addiction
- Ulcerative colitis
+ Contraindications
- Only use cannabis medicinally following the direction of a qualified medical practitioner.
- Caution with anxious or depression.
- May worsen symptoms of psychosis
- Avoid use alongside medications unless first discussing with your doctor.
+ Potential Side-Effects
- Apathy (long-term use)
- Bronchitis (smoking)
- Cough (smoking)
- Depression
- Dizziness
- Dry eyes
- Dry mouth
- Eye reddening
- Fatigue
- Hallucinations
- Headache
- Heart palpitations
- Hypertension/Hypotension
- Increased appetite
- Lightheadedness
- Menstrual changes
- Nausea/vomiting
- Numbness
- Paranoia
- Tachycardia
Herb Details: Cannabis
Weekly Dose
- (CBD content in mg)
70–700 mg - View Dosage Chart
Part Used
- Leaves, flowers, seeds
Family Name
- Cannabacea
Distribution
- Worldwide
Herbal Actions:
- Sedative/Stimulant
- Anti-emetic
- Anti-spasmodic
- Anti-convulsant
- Analgesic
- Antinflammatory
- Appetite Suppressant/Stimulant
- Adaptogen
- Anti-cancer
- Antioxidant
Common Names
- Cannabis
- Marijuana
- Hemp
- Mary Jane
- Herb
Pregnancy
- Avoid use while pregnant and nursing.
Duration of Use
- Long-term use acceptable. Recommended to take breaks periodically.
CYP450
- CYP2C9
- CYP3A4
Botanical Information
Cannabis plants are members of the Cannabacea family. This small family comprises only 11 different genuses, and about 170 species.
Some common members of the family are hops (Humulus spp.) and celtis (Celtis spp.). The celtis genus contains the largest collection of species by far, with over 100 different species. Cannabis and Humulus are the closest related genus' in the group by far.

There are three species of cannabis:
1. Cannabis sativa
Cannabis sativa is a tall, fibrous plant. It's high in cannabinoids, terpenes, and other phytochemicals — giving it many uses medicinally.
Cannabis sativa is the most commonly cultivated species. There are hundreds, if not thousands of different phenotypes of this species — the most important being hemp — which is a non-psychoactive, high fiber plant valued as both a health supplement and textile. It's also used for food (seeds), and to make biodeisel.
There are also Cannabis sativa strains high in the psychoactive component — THC — which make it popular as both medicine and recreational intoxicant.
2. Cannabis indica
Cannabis indica grows as s shorter, bushier plant. It's hgiher in THC, and there are few low-THC phenotypes available for this plant.
This species of cannabis is most often used recreationally.
3. Cannabis ruderalis
Cannabis ruderalis is a small, herbaceus plant more closely related to Cannabis sativa than Cannabis indica. It's low in cannabinoids, and terpenes, as well as fiber — limiting its value to humans.
This species has the unique ability to initiate flower production irrelevant to day length. Plant breeders have started mixing the plant with other species to gain these benefits. This makes cultivation easier in areas where day length is too short or too long for optimal cannabis cultivation.
Phytochemistry
There are 421 compounds in the cannabis plant [1], at least 66 of these are cannabinoids — some sources report as many as 112.
The top 6 cannabinoids in the plant (CBD, CBG, CNN, THC, THCV, and CBC), account for the vast majority of the cannabinoid profile.
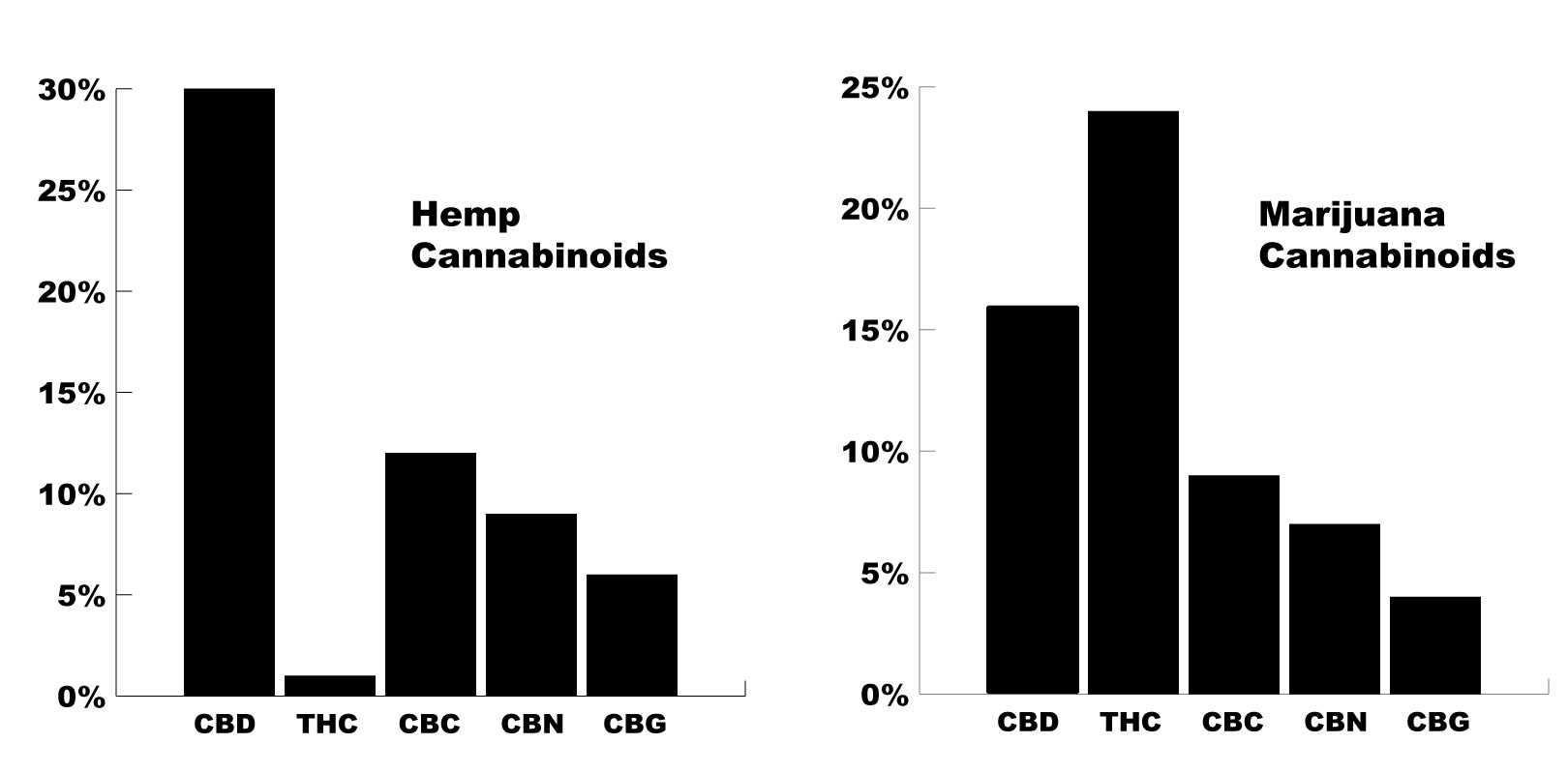
The phenotype of the cannabis used is the primary determining factor for the cannabinoid profile of each plant.
Hemp plants for example, contain much higher levels of CBD, and lower levels of THC. Marijuana strains are the opposite, contianing high THC, and lower CBD.
Depending on the strain, this can vary dramatically — and you can find almost any combination of cannabinoid possible.
The Cannabinoids:
Cannabinoids are a class of phytochemical compounds resembling the structure of our naturally occurring ecosanoid endocannabinoids; anandamide, and 2-AG. There are roughly 66 of these compounds in the cannabis plant, and a few found in other species of plants as well — such as helichrysum and echinacea.
Although the cannabinoids are very similar, their binding activity varies a lot [14]. Some bind to CB1 receptors (located primarily in the central nervous system), others bind to CB2 receptors (found primarily in immune tissue). Some cannabinoids will even bind to both, or work by increasing the concentrations of naturally occurring endocannabinoids instead.
Due to the wide range of variability between each cannabinoid, it’s useful to go over them in greater detail individually.


1. CBC
Cannabichromene
CBC is the third most abundant cannabinoid in the cannabis plant.
It’s non-psychoactive.
CBC is far less studied than the two preceding cannabinoids CBD, and THC, though early research is starting to suggest it’s even better for treating conditions like anxiety than the famed CBD.
CBC content can be increased in the cannabis plant by inducing light-stress on the plant [5].
CBC Medicinal Actions
Antidepressant
Mild sedative
Receptors Affected
Vanilloid receptor agonist (TRPV3 and TRPV4) [4]


2. CBD
Cannabidiol
In many cases, CBD is the most abundant cannabinoid. Only selectively bred cannabis strains will have higher THC concentrations than CBD.
CBD is famed for many reasons. It offers a wide range of medicinal benefits, and has been well-studied and validated over the past two decades.
CBD oils, e-liquids, and edibles have become highly popular in recent years as more of this research is being released and translated for the general public.
CBD Medicinal Actions
Antinflammatory
Mild appetite suppressant
Lowers stress
Adaptogenic
Mild sedative
Anti-emetic
Receptors Affected
Adenosine (A2a) reuptake inhibitor [6]
Vanilloid pain receptors (TRPV1, TRPV2, TRPV3) [7]
5HT1A receptor agonist (serotonin receptor) [6]
FAAH (–) [6, 7]
PPARγ nuclear receptor (+) [48]
Mg2+‐ATPase (−) [11]
Arylalkylamine N‐acetyltransferase (−) [44]
Indoleamine‐2,3‐dioxygenase (−) [45]
15‐lipoxygenase (−) [46]
Phospholipase A2 (+) [11]
Glutathione peroxidase (+) [47]
Glutathione reductase (+) [47]
5‐lipoxygenase (−) [46]
Metabolism
CYP1A1 (−) [40]
CYP1A2 & CYP1B1 (−) [40]
CYP2B6 (−) [41]
CYP2D6 (−) [42]
CYP3A5 (−) [43]



Enter KATS15 for a 15% Discount

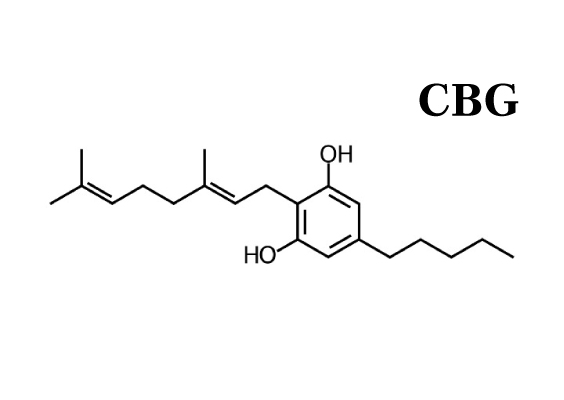
3. CBG
Cannabigerol
CBG is an early precursor for many of the other cannabinoids including THC.
Plants harvested early will be high in this compound.
Many users report that strains high in CBG are less likely to cause anxiety, and are good for people experiencing acute stress.
This is likely due to its role in blocking the serotonergic effects of THC through the 5-HT1A serotonin receptors [9].
CBG Medicinal Actions
Anti-anxiety
Adaptogenic
Mild sedative
Receptors Affected


4. CBN
Cannabinol
CBN is made from THC. As THC content breaks down with time, or heat, CBN levels increase overall.
Older harvested plants that have gone past their window of ripeness will be much higher in CBN.
It’s mostly non-psychoactive but may have some mild psychoactivity in some people.
Products or strains high in CBN will produce more of a heavy feeling and are best used for treating conditions like insomnia or anxiety.
This cannabinoid is potentially the most sedative of the group.
CBN Medicinal Actions
Sedative
Anti-anxiety
Appetite stimulant
Receptors Affected
CB1 receptor agonist [10].
Metabolism
CYP2C9

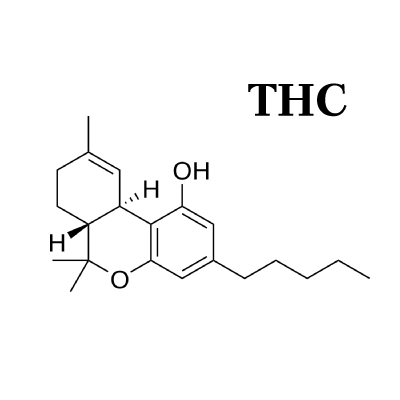
5. THC
Tetrahydrocannabinol
THC is the main psychoactive compound in the cannabis plant.
There are two main types:
Delta-8-THC — contained in very small amounts
Delta-9-THC — the most abundant form of THC in the cannabis plant
THC activates both CB1 and CB2 endocannabinoid receptors, causing changes in neurotransmitters like dopamine, norepinephrine, and most importantly, serotonin. It’s this change in neurotransmitter levels that produce the bulk of the high experienced by this compound.
Aside from its psychoactive effects, THC has medicinal benefits of its own.
It’s mentally stimulating and has some potent antidepressant effects through its euphoric effects.
THC Medicinal Actions
Appetite stimulant
Sedative (low doses)
Stimulant (high doses)
Receptors Affected
Metabolism
CYP2C9
6. THCV
Tetrahydrocannabivarin
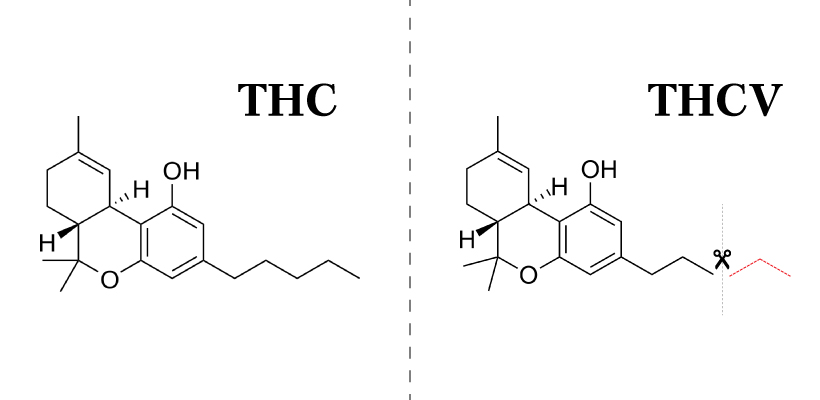
THCV is the fraternal twin of THC.
It’s virtually identical except for one slight chemical difference — THCV is missing two carbon atoms.
This makes the effects of THCV very similar to THC — but is much weaker in its effects.
One study reported THCV as being 20-25% as strong as THC in its psychoactive effects [12].
There are others affected by this, including CBCV, and CBDV, though they are in far less concentrations.

THCV Medicinal Actions
Appetite suppressant
Euphoric
Antispasmodic
Paranoic
Receptors Affected
Vanilloid receptor agonist (TRPV3 and TRPV4) [13].

7. Other Cannabinoids
There are also a lot of cannabinoids that can be found in much lower concentrations.
These make up the bottom 5% of the cannabinoid profile.
Few of these cannabinoids have many studies on them aside from chemical mapping to identify their structure.
We may see more research on these cannabinoids in the near future.
Some Novel Cannabinoids Include:
CBCV (cannabichromevarin)
CBDV (cannabidivarin)
CBE (cannabielsoin)
CBGM (cannabigerol monomethyl ether)
CBGV (cannabigerovarin)
CBL (cannabicyclol)
CBT (cannabicitran)
CBV (cannabivarin)
A Note On Synthetic Cannabinoids
There are also synthetic cannabinoids. These are compounds that are similar in shape and function to cannabinoids produced in our bodies, or in the cannabis plant.
It’s recommended that you stay far away from the synthetic cannabinoids — not only do they lack many of the medicinal actions of cannabis, they have the potential to cause serious harm.
The street drug known as “spice” is a combination of various synthetic cannabinoids. They were designed as an attempt to circumvent the legal hurdles preventing the sale of cannabis products for recreational use — and have since become a major cause of addiction and abuse.
+ Side-Effects of Synthetic Cannabinoid Use
- Agitation and anxiety
- Blurred vision
- Chest pain
- Death
- Hallucinations
- Heart attack
- High blood pressure
- Kidney failure
- Nausea and vomiting
- Paranoia
- Psychosis
- Racing heart
- Seizures
- Shortness of breath
+ List of Synthetic Cannabinoids
- JWH-018
- JWH-073
- JWH-200
- AM-2201
- UR-144
- XLR-11
- AKB4
- Cannabicyclohexanol
- AB-CHMINACA
- AB-PINACA
- AB-FUBINACA

Cannabis Terpenes
Terpenes are a class of compounds characterized by their volatile nature, and hydrocarbon-based structure. These are contained in high amounts in the essential oil of plants.
Terpenes have a very low molecular weight, and will evaporate under low temperatures. This, combined with their characteristic aromas is what gives many plants their scent. Conifer trees, fruits, and many flowers (including cannabis) all owe their aroma to their terpene profile.
Each plant can contains hundreds of different terpenes — many of which will even overlap into unrelated plant species. Cannabis shares terpenes with pine trees, many different flowers, citrus fruits, and nutmeg, among others.
Terpenes add flavor as well as additional medicinal benefits. Terpenes often have antibacterial, antiviral, antinflammatory, and anxiolytic effects.
+ List of Cannabis Terpenes
- A-humulene
- a-Terpenine
- Alpha Bisabolol
- alpha-Terpineol
- Alpha/Beta Pinene
- Beta-Caryophyllene
- Bisabolol
- Borneol
- Camphene
- Caryophyllene oxide
- D-Linalool
- Eucalyptol (1, 8 cineole)
- Geraniol
- Guaiol
- Isopulegol
- Limonene
- Myrecene
- Nerolidol
- p-Cymene
- Phytol
- Pulegone
- Terpineol-4-ol
- Terpinolene
- Trans Ocimene
- Valencene
- ∆-3-carene
Pharmacokinetics/Pharmacodynamics
Cannabinoids work by mimicking the endocannabinoids anandamide and 2-AG.

Learn more about cannabinoid metabolism.
Clinical Applications of Cannabis
As an herb, cannabis is very useful. It works through a set of receptors most other plants don’t interact with — the endocannabinoid system.
The endocannabinoid system plays a major role in maintaining homeostasis. This gives cannabis an effect profile similar to adaptogens — but through different mechanisms.
Cannabis is similar to adaptogens in that it offers a bidirectional effect profile — which means it can both increase, and decrease tissue function according to its homeostatic baseline.
But cannabis isn’t quite an adaptogen because it can’t increase the bodies resistance to stress, and doesn’t appear to exert any action on the hypothalamus or adrenal glands directly.
Although cannabis has broad actions and therefore can provide benefit to a wide range of body systems — choosing the right product, strain, and phenotype for the job is critical.
An experienced herbalist or naturopath using cannabis will take into account the cannabinoid profile, terpene content, and anecdotal effects of each strain or CBD product being used.
Unlike other herbs, you have to be very particular about the type of cannabis being used for each condition.
What Constitutes “Medicinal” Cannabis?
There’s a big difference between using cannabis because “it’s healthy”, and using it as a therapeutic agent aimed at treating a specific disease process.
Although it can be used as both, daily supplementing cannabis or extracts like CBD don’t constitute medical cannabis.
However, you can use cannabis to address the symptoms, or underlying causes for some conditions.
Cautions:
Caution advised whenever using cannabis due to the potential for intoxicating side-effects. Without careful consideration of cannabinoid profile, some strains, or cannabis products may make symptoms for certain conditions worse — especially anxiety, psychosis, bipolar disorder, and insomnia.
Recent Blog Posts:
Featured

References:
Sharma P, Murthy P, Bharath M.M.S. (2012). Chemistry, Metabolism, and Toxicology of Cannabis: Clinical Implications. Iran J Psychiatry 2012; 7:4: 149-156
Aizpurua-Olaizola, O., Soydaner, U., Öztürk, E., Schibano, D., Simsir, Y., Navarro, P., ... & Usobiaga, A. (2016). Evolution of the cannabinoid and terpene content during the growth of Cannabis sativa plants from different chemotypes. Journal of natural products, 79(2), 324-331.
Shevyrin, V. A., & Morzherin, Y. Y. (2015). Cannabinoids: structures, effects, and classification. Russian Chemical Bulletin, 64(6), 1249-1266.
De Petrocellis, L., Orlando, P., Moriello, A. S., Aviello, G., Stott, C., Izzo, A. A., & Di Marzo, V. (2012). Cannabinoid actions at TRPV channels: effects on TRPV3 and TRPV4 and their potential relevance to gastrointestinal inflammation. Acta physiologica, 204(2), 255-266.
De Meijer, E. P. M., Hammond, K. M., & Micheler, M. (2009). The inheritance of chemical phenotype in Cannabis sativa L.(III): variation in cannabichromene proportion. Euphytica, 165(2), 293-311.
Nelson, K., Walsh, D., Deeter, P., & Sheehan, F. (1994). A phase II study of delta-9-tetrahydrocannabinol for appetite stimulation in cancer-associated anorexia. Journal of palliative care.
Bisogno, T., Hanuš, L., De Petrocellis, L., Tchilibon, S., Ponde, D. E., Brandi, I., ... & Di Marzo, V. (2001). Molecular targets for cannabidiol and its synthetic analogues: effect on vanilloid VR1 receptors and on the cellular uptake and enzymatic hydrolysis of anandamide. British journal of pharmacology, 134(4), 845-852.
De Petrocellis, L., Vellani, V., Schiano-Moriello, A., Marini, P., Magherini, P. C., Orlando, P., & Di Marzo, V. (2008). Plant-derived cannabinoids modulate the activity of transient receptor potential channels of ankyrin type-1 and melastatin type-8. Journal of Pharmacology and Experimental Therapeutics, 325(3), 1007-1015.
Cascio, M. G., Gauson, L. A., Stevenson, L. A., Ross, R. A., & Pertwee, R. G. (2010). Evidence that the plant cannabinoid cannabigerol is a highly potent α2‐adrenoceptor agonist and moderately potent 5HT1A receptor antagonist. British journal of pharmacology, 159(1), 129-141.
Farrimond, J. A., Whalley, B. J., & Williams, C. M. (2012). Cannabinol and cannabidiol exert opposing effects on rat feeding patterns. Psychopharmacology, 223(1), 117-129.
Pertwee, R. G. (2008). The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Δ9‐tetrahydrocannabinol, cannabidiol and Δ9‐tetrahydrocannabivarin. British journal of pharmacology, 153(2), 199-215.
Hollister, L. E. (1974). Structure-activity relationships in man of cannabis constituents, and homologs and metabolites of Δ9-tetrahydrocannabinol. Pharmacology, 11(1), 3-11.
Pertwee, R. G. (2006). The pharmacology of cannabinoid receptors and their ligands: an overview. International journal of obesity, 30(S1), S13.
Compton, D. R., Rice, K. C., De Costa, B. R., Razdan, R. K., Melvin, L. S., Johnson, M. R., & Martin, B. R. (1993). Cannabinoid structure-activity relationships: correlation of receptor binding and in vivo activities. Journal of Pharmacology and Experimental Therapeutics, 265(1), 218-226.
Burstein, S. (2005). PPAR-γ: a nuclear receptor with affinity for cannabinoids. Life sciences, 77(14), 1674-1684.García-Arencibia, M., González, S., de Lago, E., Ramos, J. A., Mechoulam, R., & Fernández-Ruiz, J. (2007). Evaluation of the neuroprotective effect of cannabinoids in a rat model of Parkinson's disease: importance of antioxidant and cannabinoid receptor-independent properties. Brain research, 1134, 162-170.
Martín-Moreno, A. M., Reigada, D., Ramírez, B. G., Mechoulam, R., Innamorato, N., Cuadrado, A., & de Ceballos, M. L. (2011). Cannabidiol and other cannabinoids reduce microglial activation in vitro and in vivo: relevance to Alzheimers′ disease. Molecular pharmacology, mol-111.
Dirikoc, S., Priola, S. A., Marella, M., Zsürger, N., & Chabry, J. (2007). Nonpsychoactive cannabidiol prevents prion accumulation and protects neurons against prion toxicity. Journal of Neuroscience, 27(36), 9537-9544.
Malfait, A. M., Gallily, R., Sumariwalla, P. F., Malik, A. S., Andreakos, E., Mechoulam, R., & Feldmann, M. (2000). The nonpsychoactive cannabis constituent cannabidiol is an oral anti-arthritic therapeutic in murine collagen-induced arthritis. Proceedings of the National Academy of Sciences, 97(17), 9561-9566.
Specter, S., Lancz, G., & Hazelden, J. (1990). Marijuana and immunity: tetrahydrocannabinol mediated inhibition of lymphocyte blastogenesis. International journal of immunopharmacology, 12(3), 261-267.
Klein, T. W., Kawakami, Y., Newton, C., & Friedman, H. (1991). Marijuana components suppress induction and cytolytic function of murine cytotoxic T cells in vitro and in vivo. Journal of Toxicology and Environmental Health, Part A Current Issues, 32(4), 465-477.
McCoy, K. L., Gainey, D., & Cabral, G. A. (1995). delta 9-Tetrahydrocannabinol modulates antigen processing by macrophages. Journal of Pharmacology and Experimental Therapeutics, 273(3), 1216-1223.
Coffey, R. G., Yamamoto, Y., Snella, E., & Pross, S. (1996). Tetrahydrocannabinol inhibition of macrophage nitric oxide production. Biochemical pharmacology, 52(5), 743-751.
Formukong, E. A., Evans, A. T., & Evans, F. J. (1988). Analgesic and antiinflammatory activity of constituents ofCannabis sativa L. Inflammation, 12(4), 361-371.
Watzl, B., Scuderi, P., & Watson, R. R. (1991). Marijuana components stimulate human peripheral blood mononuclear cell secretion of interferon-gamma and suppress interleukin-1 alpha in vitro. International journal of immunopharmacology, 13(8), 1091-1097.
Srivastava, M. D., Srivastava, B. I. S., & Brouhard, B. (1998). Δ9 tetrahydrocannabinol and cannabidiol alter cytokine production by human immune cells. Immunopharmacology, 40(3), 179-185.
Pan, H., Mukhopadhyay, P., Rajesh, M., Patel, V., Mukhopadhyay, B., Gao, B., ... & Pacher, P. (2009). Cannabidiol attenuates cisplatin-induced nephrotoxicity by decreasing oxidative/nitrosative stress, inflammation, and cell death. Journal of Pharmacology and Experimental Therapeutics, 328(3), 708-714.
Mecha, M., Feliú, A., Iñigo, P. M., Mestre, L., Carrillo-Salinas, F. J., & Guaza, C. (2013). Cannabidiol provides long-lasting protection against the deleterious effects of inflammation in a viral model of multiple sclerosis: a role for A2A receptors. Neurobiology of disease, 59, 141-150.
Notcutt, W., Langford, R., Davies, P., Ratcliffe, S., & Potts, R. (2012). A placebo-controlled, parallel-group, randomized withdrawal study of subjects with symptoms of spasticity due to multiple sclerosis who are receiving long-term Sativex®(nabiximols). Multiple Sclerosis Journal, 18(2), 219-228.
Woerly, S., Marchand, R., & Lavallée, G. (1991). Interactions of copolymeric poly (glyceryl methacrylate)-collagen hydrogels with neural tissue: effects of structure and polar groups. Biomaterials, 12(2), 197-203.
Wade, D. T., Collin, C., Stott, C., & Duncombe, P. (2010). Meta-analysis of the efficacy and safety of Sativex (nabiximols), on spasticity in people with multiple sclerosis. Multiple Sclerosis Journal, 16(6), 707-714.
Brady, C. M., DasGupta, R., Dalton, C., Wiseman, O. J., Berkley, K. J., & Fowler, C. J. (2004). An open-label pilot study of cannabis-based extracts for bladder dysfunction in advanced multiple sclerosis. Multiple Sclerosis Journal, 10(4), 425-433.
Barnes, M. P. (2006). Sativex®: clinical efficacy and tolerability in the treatment of symptoms of multiple sclerosis and neuropathic pain. Expert opinion on pharmacotherapy, 7(5), 607-615.
Leung, L. (2011). Cannabis and its derivatives: review of medical use. The Journal of the American Board of Family Medicine, 24(4), 452-462.
Grotenhermen, F., & Müller-Vahl, K. (2012). The therapeutic potential of cannabis and cannabinoids. Deutsches Ärzteblatt International, 109(29-30), 495.
Kwiatkoski, M., Guimaraes, F. S., & Del-Bel, E. (2012). Cannabidiol-treated rats exhibited higher motor score after cryogenic spinal cord injury. Neurotoxicity research, 21(3), 271-280.
Chagas, M. H. N., Zuardi, A. W., Tumas, V., Pena-Pereira, M. A., Sobreira, E. T., Bergamaschi, M. M., ... & Crippa, J. A. S. (2014). Effects of cannabidiol in the treatment of patients with Parkinson’s disease: an exploratory double-blind trial. Journal of Psychopharmacology, 28(11), 1088-1098.
Iuvone, T., Esposito, G., De Filippis, D., Scuderi, C., & Steardo, L. (2009). Cannabidiol: a promising drug for neurodegenerative disorders?. CNS neuroscience & therapeutics, 15(1), 65-75.
Fernández‐Ruiz, J., Sagredo, O., Pazos, M. R., García, C., Pertwee, R., Mechoulam, R., & Martínez‐Orgado, J. (2013). Cannabidiol for neurodegenerative disorders: important new clinical applications for this phytocannabinoid?. British journal of clinical pharmacology, 75(2), 323-333.
Yamaori, S., Kushihara, M., Yamamoto, I., & Watanabe, K. (2010). Characterization of major phytocannabinoids, cannabidiol and cannabinol, as isoform-selective and potent inhibitors of human CYP1 enzymes. Biochemical pharmacology, 79(11), 1691-1698.
Yamaori, S., Maeda, C., Yamamoto, I., & Watanabe, K. (2011). Differential inhibition of human cytochrome P450 2A6 and 2B6 by major phytocannabinoids. Forensic Toxicology, 29(2), 117-124.
Yamaori, S., Okamoto, Y., Yamamoto, I., & Watanabe, K. (2011). Cannabidiol, a major phytocannabinoid, as a potent atypical inhibitor for cytochrome P450 2D6. Drug Metabolism and Disposition, dmd-111.
Yamaori, S., Ebisawa, J., Okushima, Y., Yamamoto, I., & Watanabe, K. (2011). Potent inhibition of human cytochrome P450 3A isoforms by cannabidiol: role of phenolic hydroxyl groups in the resorcinol moiety. Life sciences, 88(15-16), 730-736.
Yamaori, S., Ebisawa, J., Okushima, Y., Yamamoto, I., & Watanabe, K. (2011). Potent inhibition of human cytochrome P450 3A isoforms by cannabidiol: role of phenolic hydroxyl groups in the resorcinol moiety. Life sciences, 88(15-16), 730-736.
Koch, M., Dehghani, F., Habazettl, I., Schomerus, C., & Korf, H. W. (2006). Cannabinoids attenuate norepinephrine‐induced melatonin biosynthesis in the rat pineal gland by reducing arylalkylamine N‐acetyltransferase activity without involvement of cannabinoid receptors. Journal of neurochemistry, 98(1), 267-278.
Jenny, M., Santer, E., Pirich, E., Schennach, H., & Fuchs, D. (2009). Δ9-Tetrahydrocannabinol and cannabidiol modulate mitogen-induced tryptophan degradation and neopterin formation in peripheral blood mononuclear cells in vitro. Journal of neuroimmunology, 207(1-2), 75-82.
Takeda, S., Usami, N., Yamamoto, I., & Watanabe, K. (2009). Cannabidiol-2', 6'-dimethyl ether, a cannabidiol derivative, is a highly potent and selective 15-lipoxygenase inhibitor. Drug Metabolism and Disposition.
Usami, N., Yamamoto, I., & Watanabe, K. (2008). Generation of reactive oxygen species during mouse hepatic microsomal metabolism of cannabidiol and cannabidiol hydroxy-quinone. Life sciences, 83(21-22), 717-724.
Pertwee, R. G., Howlett, A. C., Abood, M. E., Alexander, S. P. H., Di Marzo, V., Elphick, M. R., ... & Mechoulam, R. (2010). International Union of Basic and Clinical Pharmacology. LXXIX. Cannabinoid receptors and their ligands: beyond CB1 and CB2. Pharmacological reviews, 62(4), 588-631.
Gymnema (Gymnema sylvestre)

What is Gymnema?
Gymnema is known as "the sugar destroyer" because of its unique ability to inhibit our ability to taste sweet foods.
This quality is used to combat sugar cravings in diabetics to control blood sugar levels.
It's been used for thousands of years in India for treating conditions involving "sweet urine." This is a common symptom of diabetes as sugar diffuses into the urinary tract. Old methods of diagnosis involved tasting the urine to identify a sweet taste.
Gymnema offers a variety of unique benefits towards conditions like diabetes, including changes to the pancreatic beta-cells, responsible for releasing insulin into the blood.
Gymnema is also a diuretic, helping to clear glucose from the blood through urine (in combination with plenty of water of course).
Finally, gymnema leaves inhibit the sweet sensation on the taste buds, making food taste bland and dull, which can be used to reduce the cravings for sweet (high sugar) foods responsible for maintaining the pathophysiology of diabetes and metabolic syndromes.
What is Gymnema Used For?
Gymnema is mainly used to treat metabolic conditions like diabetes, PCOS, and metabolic syndrome. It's also used for dental carries, and poor digestion.
+ Mechanisms
- Inreases the number of insulin-secreting beta cells in the pancreas
- Decreases the perception of sweet taste on the taste buds
- Inhibits peripheral utilization of glucose by somatotrophin and corticotrophin.
Herb Details: Gymnema
Herbal Actions:
- Antidiabetic
- Hypocholesterolemic
- Suppresses Sweet Taste
- Diuretic
- Refridgerant
- Astringent
Weekly Dose
- (1:2 Liquid Extract)
25-75 mL - View Dosage Chart
Part Used
- Leaves
Family Name
- Apocynaceae
Distribution
- Southeast Asia
Constituents of Interest
- Gymnemic acids
- Gymnemasaponins
- Gurmarin
- Betaine
Common Names
- Gymnema
- The Sugar Destroyer
- Gurmar
CYP450
- CYP3A4
- CYP2C9
- CYP1A2
- CYP2D6
Quality
- Unknown
Pregnancy
- No adverse effects expected.
Taste
- Dull (Blocks sweet receptors on the tongue)
Duration of Use
- Suitable for long term use.
Botanical Information
Gymnema is a member of the Apocynaceae (dogbane) family of plants.
In the past, gymnema was included in the milkweed (Asclepiadaceae) family — but has since been changed to a subfamily category.
The Apocynaceae family now contains 5 subfamilies (Apocynoideae, Asclepiadoideae, Periplocoideae, Rauvolfioideae, and Secamonoideae).
It contains 5100 species and 366 genera. There are roughly 50 different species of Gymnema — many of which are used interchangeably.
Many plants in the Apocynaceae family are trees preferring tropical environments — except for a handful of species that prefer to grow in deserts.
Clinical Applications Of Gymnema:
Gymnema is mainly used for metabolic conditions including hyperglycemia, hyperinsulinemia, metabolic syndrome, PCOS, hypertriglyceridemia, and both type 1 and type 2 diabetes. Its diuretic and increases the number of pancreatic beta cells.
One of the more unique effects of gymnema is its ability to inhibit sweet flavor. By simply chewing on the leaves, our ability to perceive sweet flavors gradually fades away — helping to prevent excessive sugar intake in habituated individuals.
Cautions:
High saponins may cause gastrointestinal upset, caution advised with high doses.
Caution advised if taking hypoglyemic medication due to agonistic interaction.
+ Contraindications
- Caution advised with hypoglycemic drugs
Recent Blog Posts:
Featured
As COVID-19 continues to spread around the world, we’re getting a lot of questions on what the potential role of herbal medicine is during the outbreak. Learn how the virus works and how to limit your chances of transmission.